

BACKGROUND
Autologous hematopoietic cell transplantation (AHCT) continues to be one of the most effective treatment modalities for AL amyloidosis (AL). There is a limited number of studies looking at the effect of different hematopoietic progenitor cell (HPC) mobilization regimens on HPC collection and AHCT outcomes in AL. We assessed key HPC mobilization, collection and AHCT outcomes in a cohort of AL patients.
METHODS
We conducted a retrospective cohort study of 50 AL patients (pts) who received AHCT and were mobilized with G-CSF alone (G) or G and Plerixafor (G+P) from March 2009 to April 2018. Per mobilization protocol, all pts received G four days prior to collection and P as rescue if peripheral blood (PB) CD34+ cell count was ≤20 on day 1. All patients received conditioning with high dose melphalan (140-200 mg/m2). The primary aim of the analysis was to evaluate the association of patient and disease variables (Revised Mayo stage, cardiac involvement, albumin, proteinuria, NT pro-BNP, thrombocytopenia) with HPC mobilization and AHCT outcomes (total CD34+ yield, day 1 CD34+ yield, PB CD34+, neutrophil and platelet engraftment, hospital length of stay, overall (OS) and progression-free survival (PFS)) using the two mobilization regimens. Variables were assessed relative to outcomes with Spearman correlation, Kruskal-Wallis test or Wilcoxon rank sum test. All variables were assessed relative to PFS and OS with Cox regression.
RESULTS
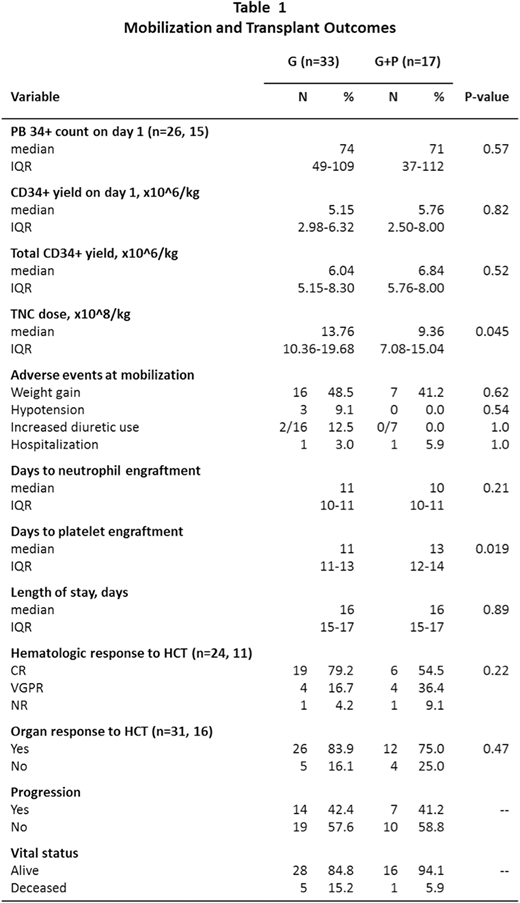
Fifty-four percent of pts were female, and median age was 60 years (range, 35-72). The majority of pts (64%) had single organ involvement (renal in 86%, cardiac in 18%). Median NT-pro BNP was 331 pg/ml (504); troponin was normal in all pts. A median of 1 line of therapy was given prior to HCT (range 0-5); 72% received cyclophosphamide, bortezomib and dexamethasone (CyBorD) (82% in G+P vs 66.7% in G cohort, p=0.33) with a median of 4 cycles prior to HCT (range 2-14). Lenalidomide-based therapy was used in 16% (29% in G+P vs 9% in G cohort, p=0.10). Thirty-three pts were mobilized with G and 17 with G+P. Relative to pts mobilized with G, those mobilized with G+P had a higher median bone marrow monotypic plasma cell % (BMPC) at diagnosis (15% in G+P vs 10% in G, p=0.029) and were older at the time of HPC collection. While the majority of pts in both groups had revised Mayo stage I AL at diagnosis, most pts with stage IV required rescue P (23% vs 3%). As shown in Table 1, there was no significant difference between the two mobilization groups with regard to the analyzed mobilization outcomes, AHCT outcomes or survival. Target collection goal of 5x10^6/kg CD34+ cells was reached in all patients within a median of 1 day (range, 1-5). Median total CD34+ yield was 6.04 (5.15-8.30)x10^6/kg with G and 6.84 (5.76-8.0) x10^6/kg with G+P. Pts who required P had a lower median collected total nucleated cell (TNC) dose (13.76 vs 9.36 x10^8/kg, p=0.045) and took 2 days longer to achieve platelet engraftment (13 vs 11, p=0.019). Pts with cardiac involvement had a lower median PB CD34+ on day 1 of collection (81 vs 48, p=0.048) but did not have a lower day 1 or total CD34+ yield. Adverse events at mobilization included weight gain, increased diuretic use, hypotension, or hospitalization and did not differ between groups. The mortality rate was 12% (6 deaths). No deaths occurred during mobilization. A higher 24-hour urine protein at diagnosis was associated with a higher mortality risk post HCT (HR 1.23, p=0.014). A higher serum albumin at diagnosis was associated with faster neutrophil engraftment (r=-0.315, p=0.026) and a signal towards a lower mortality risk however this did not reach statistical significance (HR 0.29, p=0.06). PFS and OS were similar in both groups.
CONCLUSION
In our relatively small cohort, salvage P effectively mobilized patients with low initial PB CD34 count. We found that AL patients who required rescue P (day 1 PB CD34+ cell count ≤20) had a lower TNC yield and took longer to achieve platelet engraftment speaking to suboptimal marrow reserve and possible slower engraftment kinetics. Proteinuria and potentially a low serum albumin at diagnosis may increase mortality risk post AHCT. Our study is limited by its small sample size and retrospective design. Larger cohort analyses are needed to evaluate factors associated with HPC mobilization and AHCT outcomes in AL.
Majhail:Mallinckrodt: Honoraria; Incyte: Honoraria; Nkarta Therapeutics: Honoraria; Anthem, Inc.: Consultancy. Hamilton:Syndax Pharmaceuticals: Consultancy, Honoraria. Hill:Abbvie: Consultancy, Honoraria, Research Funding; Pharmacyclics: Consultancy, Honoraria, Research Funding; AstraZenica: Consultancy, Honoraria, Research Funding; Kite, a Gilead Company: Consultancy, Honoraria, Research Funding; Novartis: Consultancy, Honoraria; BMS: Consultancy, Honoraria, Research Funding; Celgene: Consultancy, Honoraria, Research Funding; Takeda: Research Funding; Karyopharm: Consultancy, Honoraria, Research Funding; Beigene: Consultancy, Honoraria, Research Funding; Genentech: Consultancy, Honoraria, Research Funding. Jagadeesh:Regeneron: Research Funding; Debiopharm Group: Research Funding; Seattle Genetics: Membership on an entity's Board of Directors or advisory committees, Research Funding; Verastem: Membership on an entity's Board of Directors or advisory committees; MEI Pharma: Research Funding. Anwer:Incyte, Seattle Genetics, Acetylon Pharmaceuticals, AbbVie Pharma, Astellas Pharma, Celegene, Millennium Pharmaceuticals.: Honoraria, Research Funding, Speakers Bureau. Chaulagain:Sanofi Genzyme: Honoraria. Khouri:Sanofi Genzyme: Other: Advisory Board.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal